Depression: Screening and Diagnosis
Significance
- Higher prevalence of depression reported in HIV-positive persons (20-40% versus 7% in general population)
- Significant disability and poorer treatment outcomes associated with depression
Screening and Diagnosis
|
Who? |
How to screen? |
How to diagnose? |
|
Screening of all HIV-positive persons recommended in view of the high prevalence of depression Populations at particular high risk
|
1. Have you often felt depressed, sad or without hope in the last few months? 2. Have you lost interest in activities that you usually enjoy?
- Stressed, burn out, angry outbursts, coping through work or alcohol
|
Symptoms – evaluate regularly A. At least 2 weeks of depressed mood OR B. Loss of interest OR C. Diminished sense of pleasure PLUS 4 out of 7 of the following: 1. Weight change of ≥5% in one month or a persistent change of appetite 2. Insomnia or hypersomnia on most days 3. Changes in speed of thought and movement 4. Fatigue 5. Feelings of guilt and worthlessness 6. Diminished concentration and decisiveness 7. Suicidal ideation or a suicide attempti |
i. EFV has been associated with a higher risk of suicidal ideation
Depression: Management
|
Degree of depression |
No. of symptoms (A,B or + 4/7) |
Treatment |
Consultation with expert |
|
No |
<4 |
No |
|
|
Mild |
4 |
|
|
|
Intermediate |
5-6 |
Start antidepressant Treatmenti |
|
|
Severe |
>6 |
Refer to expert (essential) |
Algorithm for Diagnosis and Management of HIV-associated Neurocognitive Impairment (NCI) in Persons without Obvious Confounding Conditions
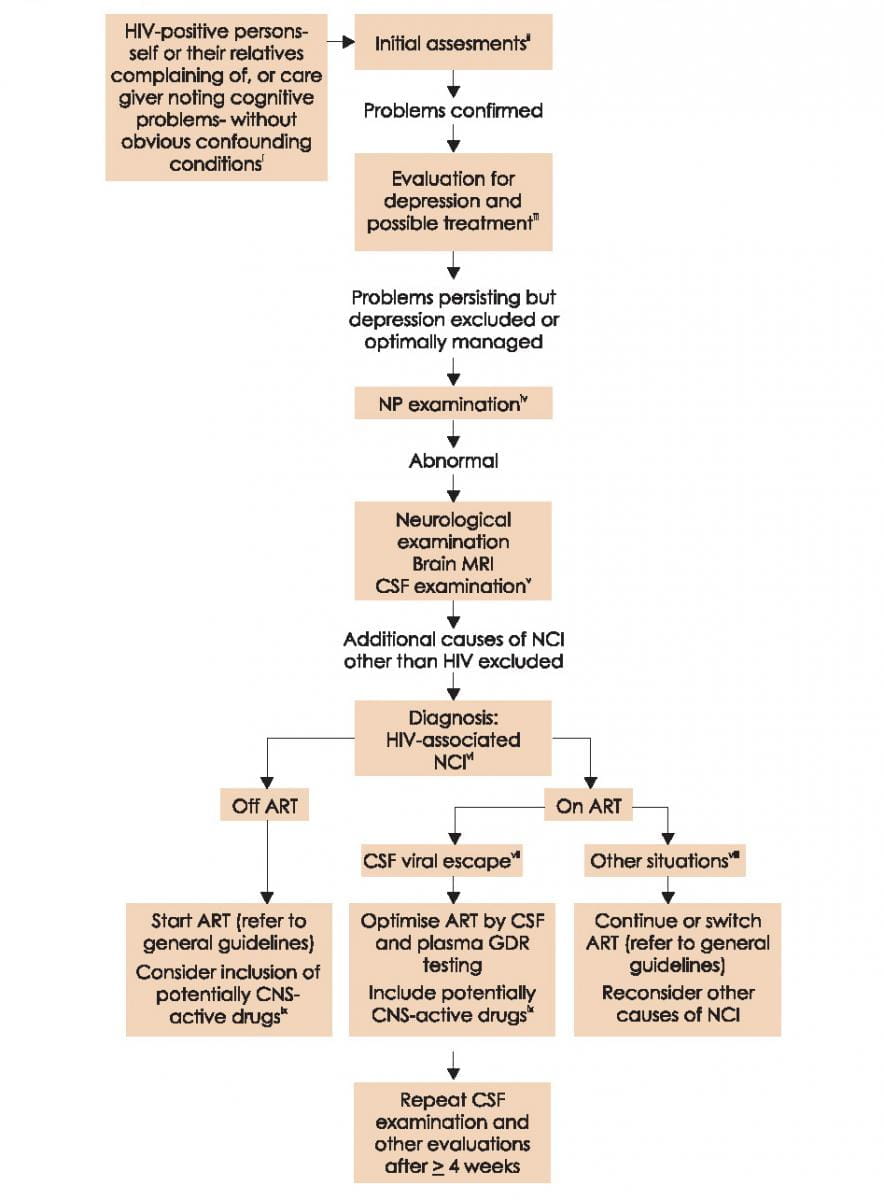
Abbreviations: CSF cerebrospinal fluid; GDR genotypic drug resistance test; HAD HIV-associated dementia; MND mild neurocognitive disorder; MRI brain magnetic resonance imaging; NP neuropsychological
- Drugs with demonstrated clear CSF penetration:
- NRTIs: ZDV, ABC*
- NNRTIs: EFV**, NVP
- PI/r, IDV/r, LPV/r, DRV/r*
- INSTI: DTG
- Other classes: MVC
- Drugs with proven clinical efficacy:
- NRTIs: ZDV, ABC
- PI/r: LPV/r
* When administered twice daily. Once-daily administration of these drugs, although common in clinical practice, has not been studied extensively with regard to CNS effects/CSF penetration and may have different CNS activity.
Classification, Doses, Safety and Adverse Effects of Antidepressants
|
Mechanisms & classification |
Start dose |
Standard dose |
Lethality in overdose |
Insomnia and agitation |
Sedati-on |
Nausea or GI effects |
Sexual Dysfuncti-on |
Weight gain |
|
mg/day |
||||||||
|
Selective serotonin-reuptake inhibitors (SSRIs)i |
||||||||
|
Paroxetine |
10-20 |
20-40 |
Low |
+ |
-/+ |
+ |
++ |
++ |
|
Sertraline |
25-50 |
50-150 |
Low |
+ |
-/+ |
+ |
+ |
+ |
|
Citalopram |
10-20 |
20-40 |
Low |
+ |
-/+ |
+ |
+ |
+ |
|
Escitalopram |
5-10 |
10-20 |
Low |
+ |
-/+ |
+ |
+ |
+ |
|
Mixed or dual-action reuptake inhibitors |
||||||||
|
Venlafaxine |
37.5-75 |
75-225 |
Moderate |
++ |
-/+ |
+ |
+ |
-/+ |
|
Mixed-action newer agents |
||||||||
|
Mirtazapine |
30 |
30-60 |
Low |
-/+ |
++ |
-/+ |
-/+ |
++ |
- None
+ Moderate
++ Severe
i For many persons, SSRI induction may be associated with adverse effects (GI tract, dizziness, anxiety, panic attacks). Commencing at lower doses (i.e. 10, 25 & 10 mg for Paroxetine, Sertraline and Citalopram, respectively) and increasing to the above starting doses after 4 to 7 days, if tolerated, may reduce such effects.
Drug-drug Interactions between Antidepressants and ARVs
|
Antidepressants |
ATV/r |
DRV/c |
DRV/r |
LPV/r |
EFV |
ETV |
NVP |
RPV |
MVC |
DTG |
EVG/c |
RAL |
|
|
SSRI |
citalopram |
↑a |
↑ |
↑ |
↑a |
↓ |
↓ |
↓ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
escitalopram |
↑a |
↑ |
↑ |
↑a |
↓ |
↓ |
↓ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
fluvoxamine |
↑ |
↑ |
↑ |
↑ |
↔ |
↔ |
E |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
fluoxetine |
↑ |
↑ |
↑ |
↑ |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
paroxetine |
↑↓? |
↑↓? |
↓39% |
↑↓? |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑↓? |
↔ |
|
|
sertraline |
↓ |
↑ |
↓49% |
↓ |
↓39% |
↓ |
↓ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
SNRI |
duloxetine |
↑↓ |
↑ |
↑↓ |
↑↓ |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
venlafaxine |
↑ |
↑ |
↑ |
↑ |
↓ |
↓ |
↓ |
↔ |
D |
↔ |
↑ |
↔ |
|
|
TCA |
amitriptyline |
↑a |
↑ |
↑ |
↑a |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
clomipramine |
↑a |
↑ |
↑ |
↑a |
↓ |
↓ |
↓ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
desipramine |
↑a |
↑ |
↑ |
↑5%a |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
doxepin |
↑ |
↑ |
↑ |
↑ |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
imipramine |
↑a |
↑ |
↑ |
↑a |
↓ |
↓ |
↓ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
nortriptyline |
↑a |
↑ |
↑ |
↑a |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
trimipramine |
↑ |
↑ |
↑ |
↑ |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
TeCA |
Maprotiline |
↑ |
↑ |
↑ |
↑ |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
mianserine |
↑ |
↑ |
↑ |
↑ |
↓ |
↓ |
↓ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
mirtazapine |
↑ |
↑ |
↑ |
↑ |
↓ |
↓ |
↓ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
|
Others |
bupropion |
↓ |
↔ |
↓ |
↓57% |
↓55% |
↔ |
↓ |
↔ |
↔ |
↔ |
↑? |
↔ |
|
lamotrigine |
↓32% |
↔ |
↓ |
↓50% |
↓ |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
↔ |
|
|
nefazodone |
↑ |
↑ |
↑ |
↑ |
↓E |
↓E |
↓E |
E |
E |
↔ |
↑ |
↔ |
|
|
St. John’s wort |
D |
D |
D |
D |
D |
D |
D |
D |
D |
Db |
D |
↔ |
|
|
trazodone |
↑ |
↑ |
↑ |
↑ |
↓ |
↓ |
↓ |
↔ |
↔ |
↔ |
↑ |
↔ |
|
↑ potential elevated exposure of the antidepressant
↓ potential decreased exposure of the antidepressant
Reference
EACS Guidelines version 8.0 - October 2015