

Effect of Long-term Azithromycin Treatment on Airway Wall Thickness in Patients with SPA

25 Nov, 21


Introduction
Severe persistent asthma (SPA) is a subset of difficult-to-treat asthma that remains uncontrolled despite treatment with high-dose inhaled corticosteroids plus a second controller and (or) systemic corticosteroids, or that worsens when high-dose treatment is decreased.
Aim
To study the effect of long-term treatment with azithromycin on airways wall thickness in patients with severe persistent asthma (SPA)
Patient Profile
Adult (18-65 years) patients with severe persistent asthma
Methods
- Randomized, double-blind, placebo-controlled clinical trial
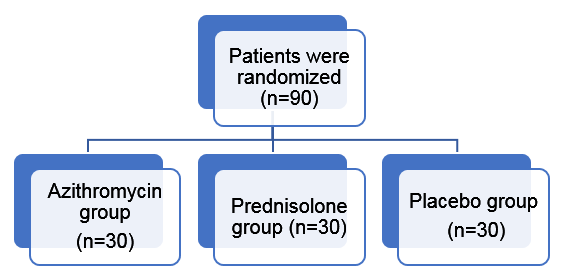
- Study drugs
- Azithromycin (250 mg, BID, three days a week)
- prednisolone (5 mg, BID), or
- placebo for eight months in three separate groups in addition to the standard therapy
Treatment duration: 8 months
Study Outcome
- Primary Outcome: The improvement in right upper lobe apical segmental bronchus (RB1) wall thickness obtained by high resolution computed tomography was set as the primary outcome
- Secondary outcomes: Cough severity, dyspnea severity, asthma control test (ACT) score, asthma exacerbation rate, pulmonary function tests, and fractional exhaled nitric oxide (FENO)
Results
- Bronchial wall thickness percentage did not change significantly in any of the groups
- The inner radius and lumen area of azithromycin and prednisolone-treated subjects increased significantly (p < 0.05 for both)
- Cough, dyspnea severity and Asthma exacerbation rate (AER)
- Azithromycin also significantly improved the dyspnea severity, ACT score, FENO, and FEV1, FEF25-75, and FEV1/FVC (p < 0.05 for all)
- Cough severity or asthma exacerbation rate did not change significantly after eight months of treatment with azithromycin
- The frequency of patients with improved dyspnea severity in the azithromycin group (n = 18) was significantly more than the placebo group (n = 5, p < 0.001)
- Post-treatment AER were 2 [Q1 = 1.5 - Q3 = 3], 2 [Q1 = 1 - Q3 = 2], and 2 [Q1 = 0 - Q3 = 2] for azithromycin, prednisolone, and placebo groups, respectively.
- Median survival days (days without any asthma exacerbation) in azithromycin, prednisolone, and placebo groups were 279, 300, and 205 days, respectively
- ACT score
- Azithromycin and prednisolone groups had a significant increase in the ACT scores (p < 0.001 for both).
- The mean change of ACT score from baseline in the azithromycin group (3.52 ± 2) was significantly less than the prednisolone group (6.2 ± 2.2) but significantly more than the placebo (0.7 ± 2.4) group (p < 0.001 for both)
- FENO
- Post-treatment FENO was 23 [Q1 = 11 - Q3 = 83.5], 22 [Q1 = 7 - Q3 = 80], and 28.5 [Q1 = 19 - Q3 = 42.25] in azithromycin, prednisolone, and placebo groups, respectively
- FENO in azithromycin and prednisolone groups reduced significantly (p < 0.05 for both)
- Lung function
- FEV1, FEV1/FVC, and FEF25-75 increased significantly in both azithromycin and prednisolone groups (p < 0.05 for all)
- Safety
- No significant difference in the frequency of adverse events, serious adverse events, or adverse events leading to discontinuation of the study drug were observed (p > 0.05 for all)
Conclusion
- Long-term treatment with azithromycin demonstrated increased lumen radius and lumen area in patients with severe persistent asthma
- The study highlighted the ability of azithromycin in improving clinical findings, including dyspnea severity, ACT score, and pulmonary function tests
- The data suggest that azithromycin is a potentially useful add-on treatment option in patients with SPA, but it has no effect on airway wall thickness
Reference
Respiratory Medicine.2021;185:106494
Related Topics
More From Area Of Interest
You may also like

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
29 Apr, 26

29 Apr, 26
Journal Scans
29 Apr, 26

29 Apr, 26
Journal Scans
29 Apr, 26

29 Apr, 26


