Introduction
Dermatophytosis is a prevalent problem in developing countries like India due to its hot and humid climate. In addition, there may be other factors affecting the prevalence of dermatophytosis. Despite the high incidence and clinical relevance, multicentric evidence depicting the present-day clinico-epidemiological patterns of dermatophytosis across India is scarce.
Aim
To assess the prevalence of pathogenic dermatophytes, clinical types of dermatophyte fungal infection, and in vitro antifungal drug susceptibility testing against dermatophytes
Patient Profile
- Patients with clinically suspected dermatophytosis of the skin
- Aged between 18 and 65 years
Methods
- Cross-sectional, multicentric study,
- 395 patients with dermatophytosis from five cities across India ((Mumbai, Delhi, Kolkata, Lucknow and Hyderabad) were enrolled
- All patients were subjected to clinical examination and investigations including direct microscopic examination with 10% KOH (Potassium Hydroxide), fungal culture and antifungal susceptibility tests
- Antifungal drug susceptibility testing was performed as per the microbroth dilution technique of Clinical and Laboratory Standards Institute Guidelines
- The antifungal drug susceptibility testing was done for seven antifungal agents, namely, luliconazole, sertaconazole, eberconazole, itraconazole, terbinafine, griseofulvin and amorolfine
Results
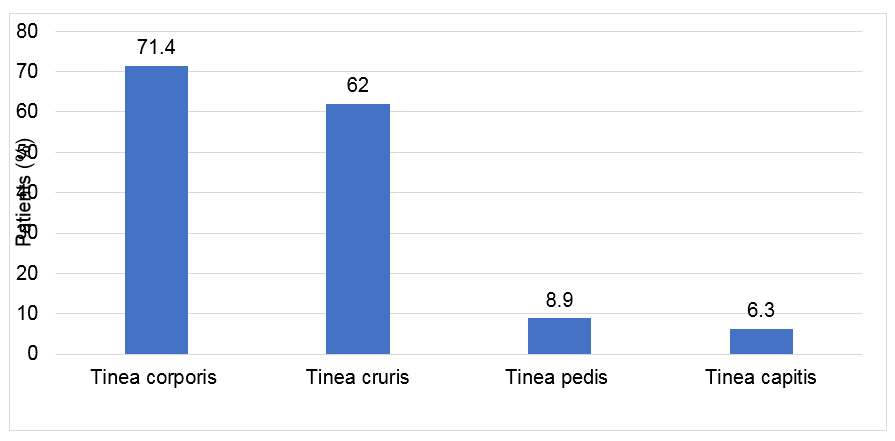
- The clinical types of dermatophytosis are as mentioned in Figure 1. Tinea corporis and tinea cruris were the common clinical presentations.
- The distribution of the fungal isolates is given in Table 1. Among dermatophytes, the genus Trichophyton represented the majority of the isolates of dermatophytes.
- T. rubrum was the most predominant fungal isolate (68.4%) followed by T. mentagrophytes (29.3%)
- Within species, T. mentagrophytes was prevalent in humid environmental conditions (Mumbai and Kolkata), whereas T. rubrum was prevalent in noncoastal areas (Delhi, Lucknow and Hyderabad)
Table 1: Distribution of fungal isolates
|
Species |
Gender |
Age Group | ||
|
|
Male (n=109) (%) |
Female (n=65) (%) |
18–50 (n=137) (%) |
>50 years (n=37) (%) |
|
Trichophyton rubrum |
77 (70.6) |
43 (64.6) |
97 (70.8) |
22 (59.5) |
|
Trichophyton mentagrophytes |
30 (27.5) |
21 (32.3) |
37 (27.0) |
14 (37.8) |
|
Trichophyton tonsurans |
2 (1.8%) |
0 |
1(0.7%) |
1 (2.7%) |
|
Microsporum canis |
0 |
1 (1.5%) |
1(0.7%) |
0 |
|
Trichophyton rubrum var. granulare |
0 |
1 (1.5%) |
1(0.7%) |
0 |
- Antifungal drug susceptibility testing results are given in Table 2. Data indicated that griseofulvin had the least mean minimum inhibitory concentration (MIC) values, followed by luliconazole, eberconazole, sertaconazole, amorolfine and itraconazole.
- Among oral antifungals, the mean MIC of itraconazole was within the range (0.84 [0.252] µg/ mL). High mean MIC values were reported for terbinafine (0.05 [0.043] µg/mL). However, it was noted only in 20 (11.5%) out of total culture-positive patients.
- Among topical antifungals, luliconazole presented the lowest mean MIC values across different regions, followed by eberconazole and amorolfine.
- All 174 (100%) patients were susceptible to griseofulvin, itraconazole, luliconazole, sertaconazole, amorolfine and eberconazole.
|
Category |
Culture positive (n = 174) |
|
Terbinafine |
|
|
High MIC |
20 (11.5%) |
|
Susceptible |
154 (88.5%) |
|
MIC (µg/mL), mean (SD) |
0.05 (0.043) |
|
MIC90 |
0.001–0.03 |
|
Griseofulvin |
|
|
High MIC |
0 (0.0%) [NE] |
|
Susceptible |
174 (100.0%) |
|
MIC (µg/mL), mean (SD) |
0.19 (0.082) |
|
MIC90 |
0.25–3.0 |
|
Itraconazole |
|
|
High MIC |
0 (0.0%) [NE] |
|
Susceptible |
174 (100.0%) |
|
MIC (µg/mL), Mean (SD) |
0.84 (0.252) |
|
MIC90 |
0.05–1.0 |
|
Luliconazole |
|
|
High MIC |
0 (0.0%) [NE] |
|
Susceptible |
174 (100.0%) |
|
MIC (µg/mL), Mean (SD) |
0.29 (0.286) |
|
MIC90 |
0.05–1.0 |
|
Sertaconazole |
|
|
High MIC |
0 (0.0%) [NE] |
|
Susceptible |
174 (100.0%) |
|
MIC (µg/mL), Mean (SD) |
0.36 (0.372) |
|
MIC90 |
0.05–1.0 |
|
Amorolfine |
|
|
High MIC |
0 (0.0%) [NE] |
|
Susceptible |
174 (100.0%) |
|
MIC (µg/mL), Mean (SD) |
0.60 (0.306) |
|
MIC90 |
0.05–1.0 |
|
Eberconazole |
|
|
High MIC |
0 (0.0%) [NE] |
|
Susceptible |
174 (100.0%) |
|
MIC (µg/mL), Mean (SD) |
0.32 (0.251) |
|
MIC90 |
0.05–1.0 |
|
NE: Not estimable |
|
Conclusion
- T. rubrum was the most common, followed by T. mentagrophytes as an emerging/codominant fungal isolate in India
- Tinea corporis was the most common clinical type of dermatophytosis
- Mean MIC of terbinafine was above the reference range, while it was within the range for itraconazole; griseofulvin had the lowest mean MIC.
- Luliconazole presented the lowest mean MIC values across different regions.
Reference
Indian J Dermatol Venereol Leprol 2021;87:800-6.