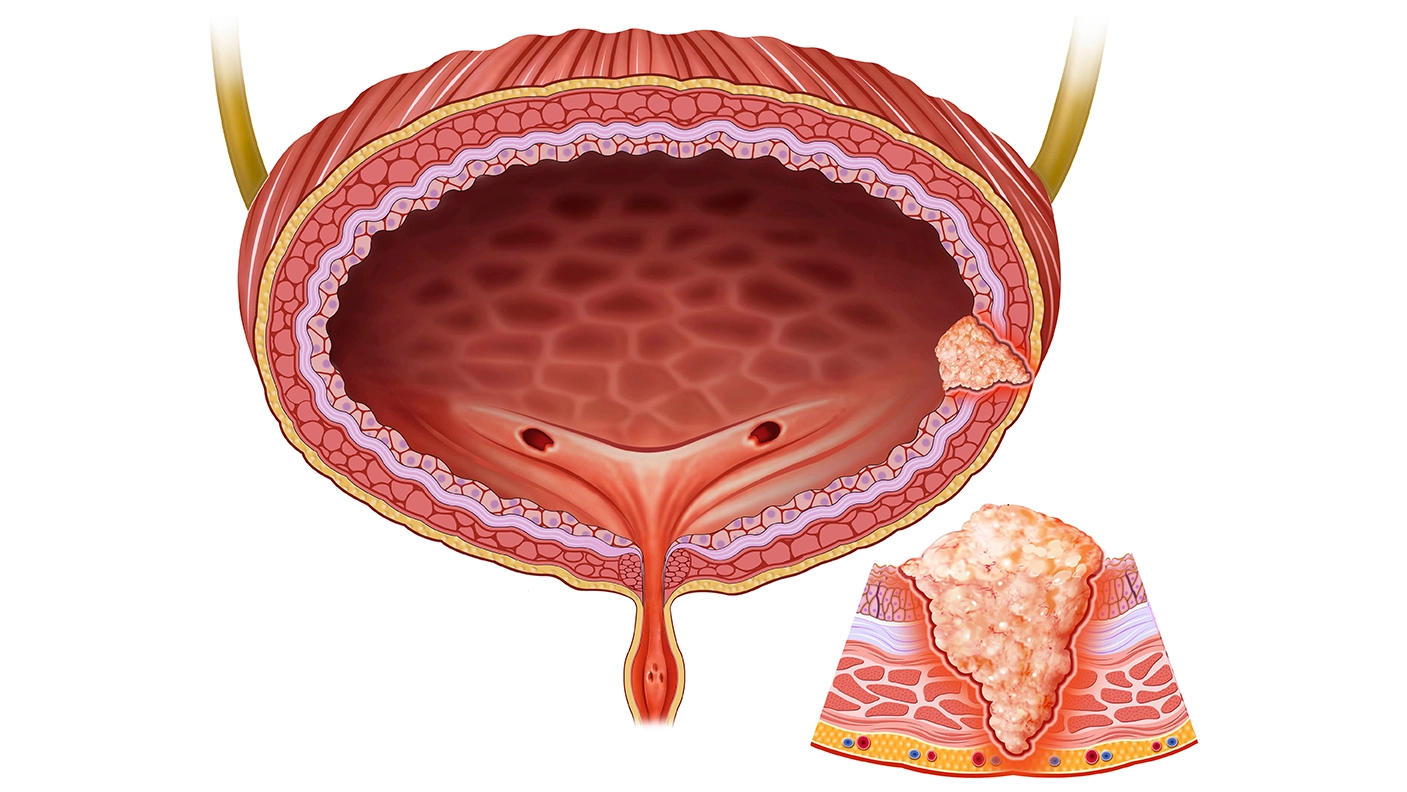
EAU 2024: Discussion Bladder Cancer






Extended Lymphadenectomy for BC is Not Necessary Pros- By Prof. Juergen E.
Gschwend
The speaker, Professor Gschwend, presented on the topic of extended lymphadenectomy for bladder cancer during a conference. The speaker highlighted that the extent of lymph node dissection in bladder cancer patients undergoing radical cystectomy could impact survival, citing various retrospective studies. He then discussed the German LEA-AUO trial, the first prospective randomized clinical trial comparing standard and extended pelvic lymph node dissection, published in 2019, with follow-up data presented in 2023. In the trial, standard lymphadenectomy involved six fields in the small pelvis, while extended dissection encompassed 14 fields up to the AMI. The trial included patients with invasive, locally resectable urothelial bladder cancer who had not undergone neoadjuvant chemotherapy. The primary endpoint was time to progression, with overall survival and cancer-specific survival as secondary endpoints. A consort diagram illustrated the randomization of 401 patients evenly between the standard and extended lymph node dissection groups.
The study delineates patient characteristics, emphasizing the notable abundance of removed lymph nodes within the limited field, with a median count of 19 lymph nodes ranging from 2 to 66, contrasting with the extended field's median count of 31 lymph nodes. Consequently, the trial aimed to juxtapose the efficacy of rather extended versus super extended lymph node dissection. Notably, approximately 50 percent of patients presented with lower-risk disease, categorized as T2 or less, while 25 percent exhibited node-positive disease, aligning closely with findings from significant cystectomy series. Post-radical cystectomy, approximately 14-15 percent of patients underwent adjuvant chemotherapy, reflecting current treatment paradigms.
The primary analysis focused on recurrence-free survival, the primary endpoint of the study, revealed a difference that did not reach statistical significance. The hazard ratio was observed at 0.83, with a five-year recurrence-free survival rate of 61% compared to 67%. Furthermore, cause-specific survival, a critical secondary endpoint, indicated a more pronounced difference, with a five-year survival rate of 76% compared to 65%. Despite a favourable hazard ratio of 0.7, statistical significance was not achieved. Several factors contributed to this outcome, including insufficient statistical power due to the study's sample size of 400 patients.
The study examined complications arising from lymphocele formation within 30- and 90 days post-operation, comparing outcomes between limited and extended fields. Results indicated a higher incidence of lymphocele in the extended field group, with a prevalence of approximately 7-8% compared to 2-3% in the limited field group. No significant variance in severe complications was observed between the two fields aside from the noted disparity in lymphocele occurrence.
At the ASCOR meeting last year, Seth Lerner presented the SWOG trial, which had been eagerly awaited. The trial incorporated neoadjuvant chemotherapy, distinguishing it from previous efforts. Nonetheless, the trial revealed no advantage in extending lymph node dissection compared to the standard approach. The finding echoes discussions held at the EAU presentation, where a secondary analysis was conducted after nearly five years of follow-up. Although the initial difference in time to progression was not statistically significant at 8 percent, a notable divergence in long-term cancer-specific survival emerged. While this parameter was not the primary endpoint, it represented a key secondary outcome, revealing a significant 12 percent disparity between extended and standard lymph node dissection, thereby achieving statistical significance.
In conclusion, the analysis of extended lymph node dissection compared to standard lymph node dissection for the primary endpoint of time to progression yielded no significant advantage, particularly evident in both the LEA and SWOG trials. Conversely, an improvement in core-specific survival as a secondary endpoint was notable with prolonged follow-up, signifying potential significance for patients. This underscored the pivotal importance of the quality of lymph node dissection during radical cystectomy. Thus, it is imperative to conduct thorough and safe lymphadenectomy procedures. However, it is crucial to note that higher lymph node counts do not inherently equate to better outcomes.
Extended Lymphadenectomy for Bladder Cancer is Not Necessary CON: By Dr Rafael Sanchez-Salas
The speaker focused on delineating three distinct lymphoid dissection templates: limited, extended, and super extended, each represented by different colour codes for clarity. Reference is made to Donald Skinner's assertion from 1982 emphasizing the importance of meticulous lymph node dissection in potentially influencing outcomes. The speaker underscores the critical roles played by both operating urologists and examining pathologists in ensuring the thoroughness and accuracy of lymph node evaluation, particularly concerning the detection of micro-metastatic disease. It is noted that standard lymph node dissection enables accurate staging in a majority of cases, with only a minimal number of positive lymph nodes potentially missed. However, opting for an extended dissection, encompassing areas such as the common iliac or aortic bifurcation, substantially increases the likelihood of identifying additional positive lymph nodes, particularly in cases of positive disease. The range of positivity rates associated with extended lymphadenectomy is highlighted, further underscoring its potential significance in disease management.
The LEA trial, as elucidated by Dr. Gschwend, entailed 458 randomized patients, with actual randomization occurring among 401 patients. The trial offered exceedingly comprehensive data, emblematic of German quality standards. Nevertheless, no discernible disparities surfaced in terms of recurrence-free survival, cancer-specific survival, or overall survival. Noteworthy details included a 5.5 percent variance in recurrence-free survival, conceivably attributable to the 15 percent power threshold. This discrepancy may have stemmed from the absence of a predefined template, replaced instead by a cutoff of 15 lymph nodes, potentially influencing outcomes. Moreover, the trial encompassed 14 percent of T1G3 disease cases, characterized by a minimal risk of nodal involvement. Furthermore, 56 percent of PT2 disease cases were included, also featuring a low risk of non-standard nodal involvement. Notably, no adjuvant chemotherapy was administered, although a considerable proportion of patients exhibited positive surgical margins, a factor likely to have impacted results. Additionally, adjuvant chemotherapy was provided to 20 percent of patients post-surgery. While the trial's graphical representations revealed extended and limited curves lacking clinical significance, Dr Gschwend underscored the attainment of statistical significance over time, a pivotal observation.
The speaker also referenced Dr. Seth Lerner’s SWOG trial, which entailed a randomization comparing standard versus extended procedures. This randomization was based on a projected 53% benefit in cancer-free survival at three years, with an 85% statistical power. The sample size exceeded that of the LEO trial, with an assumed 10% possibility of non-randomization after a six-year follow-up period. However, the SWOG trial did not demonstrate a benefit for extended lymph node dissection but rather revealed an increased risk of side effects and postoperative mortality. Thus, the speaker emphasized the importance of the procedural template, as randomization was conducted intraoperatively, necessitating documentation of surgical performance for evaluation by Dr. Lerner. Notably, the absence of T1G3 disease in the trial's inclusion criteria likely contributed to a more homogeneous selection process. Additionally, neoadjuvant chemotherapy was administered to 56% of patients in the trial. While a direct comparison of survival curves may not be appropriate, their overlapping nature suggests a lack of benefit from the extended procedure.
When examining the trials, it seemed that there was perhaps no benefit. However, upon analyzing the pre-specified comparisons of disease-free survival treatments and considering patients with prior PT three and PT four diseases, a difference might have emerged. This suggested that opting for lymph node dissection might not have been a bad idea. Furthermore, when comparing the LEA trial and the SWOG trial, a notable discrepancy was observed. It was evident that an intraoperative decision could have made a significant difference between an extended or a standard dissection.
In conclusion, an extended lymph node dissection was found not to be associated with improved survival based on the initial retrieval. The results of both the LEA and the most recent findings from the SWOG trial underscored the importance of careful patient selection. The standard approach, namely the standard dissection, was considered the gold standard. However, extended lymph node dissection might have had a role in select patients. As Dr. Lerner stated, if nodes were observed in the extended template, an extended node dissection would be performed. Thus, the decision was based on individual case selection.
Role of Immunotherapy of Bladder Cancer: By Marko Babjuk
The speaker addressed the potential of immunotherapy in treating urothelial carcinoma, emphasizing its suitability due to the tumor's high mutation frequency, which results in increased antigen presentation to the immune system. He highlighted that while checkpoint inhibitors are commonly discussed, both passive and active immunotherapy methods are also considered. In the context of muscle-invasive tumors, the speaker noted the role of BCG as a nonspecific immunotherapy and discussed the upregulation of the PD-1 receptor or PDL-1 ligand on tumor cells to enhance the immune response against cancer. Current treatments for muscle-invasive tumors, particularly for metastatic or advanced disease, include avelumab and checkpoint inhibitors. However, these treatments are often palliative. The speaker proposed extending immunotherapy to non-muscle invasive tumors, especially for patients at risk of progression. He mentioned potential resistance mechanisms to BCG, such as PD-L1 upregulation on bladder cancer cells, and suggested combining local and systemic immunotherapy for these patients.
The speaker referred to ongoing trials for high-risk disease patients and mentioned the results of the KEYNOTE 057 trial, which evaluated systemic pembrolizumab in BCG-unresponsive carcinoma in situ patients. The trial demonstrated a 40% complete response rate, leading to FDA approval. However, the treatment is not widely used due to notable side effects. Data on atezolizumab showed similar efficacy but with significant toxicity. The speaker highlighted preliminary data from the ADAPT trial, which combined systemic durvalumab with BCG or external radiation. Particularly when durvalumab was combined with BCG, the results were promising.
The speaker stated that several ongoing trials are investigating protocols combining systemic and local immunotherapy in patients with BCG and those who are BCG naive. Preliminary results from these trials are anticipated to be interesting. Additionally, there are efforts to use checkpoint inhibitors in combination with intravesical treatments. A phase-1 trial published in European Urology suggests this approach is feasible but has some associated toxicity. Alternative approaches, such as oncolytic viruses, are also being explored, particularly in combination with BCG. The speaker mentioned the interleukin super agonist N803, which, combined with intravesical BCG, has shown promising results with a complete response rate of over 70%.
Another innovative approach is gene therapy using Nadofaragene Firadenovec (Adstriladrin), which transfers the interferon gene intravesically, stimulating interferon production by urothelial and tumor cells. Interferon has demonstrated anti-tumor efficacy, and the bladder wall has been shown to produce interferon for approximately 10 days following this treatment. This therapy requires installation only once every three months and has shown promising results in BCG-unresponsive CIS patients, with a response rate exceeding 50%. This drug received approval for BCG-unresponsive patients over a year ago.
In conclusion, the speaker emphasized that this is an exciting area of research, with checkpoint inhibitors playing a significant role in advanced urothelial cancer. It is anticipated that the role of checkpoint inhibitors and other immunotherapies will expand to include non-muscle-invasive tumors, promising even more potential in the future.
Discussion
During the discussion, the question was raised that only a minimal amount of neoadjuvant chemotherapy was used in the German trial. However, there are possibilities to go further, such as using Vedotin, which might be more effective. The inquiry raised was whether there is still a need to debate the use of systemic therapy given its efficacy. Prof. Juergen E. Gschwend responded by stating that the field is rapidly evolving, and it's uncertain what will be considered standard neoadjuvant chemotherapy in the next few years. Currently, neoadjuvant chemotherapy is the standard of care. However, many patients do not receive it before undergoing a regular cystectomy. He is unsure if this will change in the future, especially with options like EV Pembro being expensive and not universally accessible. Prof. Gschwend emphasizes the importance of surgical quality in treating muscle-invasive bladder cancer, regardless of neoadjuvant chemotherapy use. While he advocates for neoadjuvant treatment, he acknowledges its limited adoption, even in Western countries like Germany.
Two recent trials yielded negative results, but there's potential for a turnaround. The argument revolves around the value of extensive lymphadenectomy for the T3 and T4 stages of the disease. While initial indications pointed towards T3 and T4, a post hoc analysis by Jürgen Gschwend and the German group suggested that T2 might benefit more from extensive lymphadenectomy. Dr. Rafael Sanchez-Salas emphasizes that a post hoc analysis is unplanned and should be viewed with caution. He acknowledges limitations in the trial's inclusion criteria, noting that a high percentage of T2 patients benefited from the intervention due to the nature of the disease and the importance of primary treatment. Dr. Sanchez-Salas agrees with Dr. Gschwend that selective treatment approaches are needed. This would involve determining which patients would benefit from neoadjuvant chemotherapy, primary treatment bladder cystectomy, or a trimodal organ preservation approach. When asked about the superiority of one trial over the other, Dr. Sanchez-Salas refrains from making a definitive judgment. He acknowledges the high quality of the German trial and the longevity of the SWOG trial but emphasizes the importance of the surgeon's experience and judgment in deciding on lymphadenectomy.
During a discussion, Marko Babjuk was queried about the role of surgery quality in immunotherapy and whether additional information from specimens could aid in immunotherapy selection. Marko Babjuk mentioned that currently, surgery quality might not heavily influence immunotherapy outcomes. However, he emphasized the importance of high-quality lymph node dissection, citing diverse practices among institutions. He suggested that the future lies in more selective approaches, as not all patients benefit from current treatments due to a lack of individualization. Babjuk proposed the need for better patient selection based on tissue markers, specifically from transurethral resection rather than cystectomy specimens.
European Association of Urology (EAU) Annual Congress 2024, 5th April - 8th April 2024, Paris, France