Risk Stratification in PAH with a Comprehensive Echocardiographic Method



Introduction
Currently approved pulmonary arterial hypertension (PAH) therapies should be initiated based on the risk stratification as per the recommendations from the 6th World Symposium on Pulmonary Hypertension. However, the current parameters as recommended by 2015 ERS/ESC and REVEAL RISK SCORE 2.0, use a broad range of invasive and non-invasive parameters to assess the mortality risk of PAH patients such as WHO functional class (WHOFC), 6-min walk distance (6MWD), hemodynamics, cardiopulmonary exercise testing, N-terminal (NT)-pro hormone BNP levels, imaging, catheterization (RHC), they are of insufficient prognostic value in terms of achieving the treatment goals in PAH. A comprehensive echocardiographic assessment of right ventricular (RV) function would be highly valuable in the risk stratification of PAH patients.
Aim
This study evaluates whether the incorporation of multiple parameters reflecting right heart function could improve the prognostic value of this imaging modality.
Methods
Study Design
- Pooled data analysis from 7 observational studies that evaluated the prognostic value of echocardiography in PAH patients
Treatment Strategy
- A total of 517 patients were recruited and classified into 3 groups representing progressive degrees of RV dysfunction based on a combination of echocardiographic measurements
- Group 1: normal tricuspid annular plane systolic excursion (TAPSE) and non-significant tricuspid regurgitation (TR); low risk
- Group 2: normal TAPSE and significant TR; intermediate risk
- Group 3: impaired TAPSE without systemic congestion; intermediate risk
- Group 4: impaired TAPSE associated with systemic congestion; high risk
Endpoints
- 5-year survival rates
Results
- Cohort comprised 517 patients with mean age 52+15 years and 64.8% females
- The number of patients in the 4 groups are shown in figure 1.

- There were 206 deaths (39.8%) during the median follow-up of 46 months
- The survival rates are compared in figure 2.
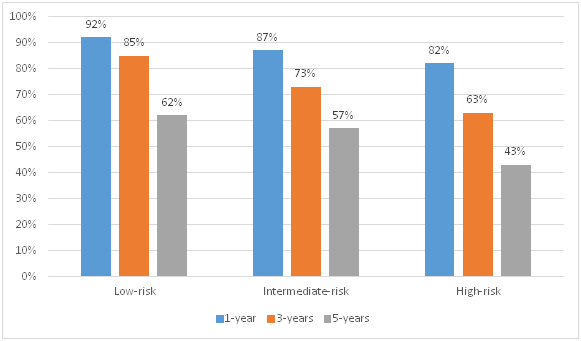
- The survival outcomes of low-risk patients were better than intermediate-risk patients (log-rank ?2: 12.25 p<0.001) and intermediate-risk patients had better survival outcomes than high-risk patients (log-rank ?2: 26.25 p<0.001).
- There was no addition in the prognostic value after inclusion of other parameters such as right atrial area and pericardial effusion
Conclusion
- Integration of the echocardiographic parameters such as tricuspid annular plane systolic excursion (TAPSE), tricuspid regurgitation (TR) grade and inferior vena cava (IVC) was effective in stratifying the risk for all-cause mortality in pulmonary arterial hypertension (PAH) patients.
- This echocardiographic approach outperformed the parameters suggested by 2015 ERS/ESC guidelines.
Eur Respir J 2020. Doi: 10.1183/13993003.00513-2020.